
Accidents and injuries statistics – Statistics Explained
,_residents,_2020_Health2023.png/800px-Causes_of_death_–_accidents_(including_the_sequelae_of_transport_and_other_accidents),_residents,_2020_Health2023.png "Accidents and injuries statistics – Statistics Explained")
Deaths from accidents, injuries and assault
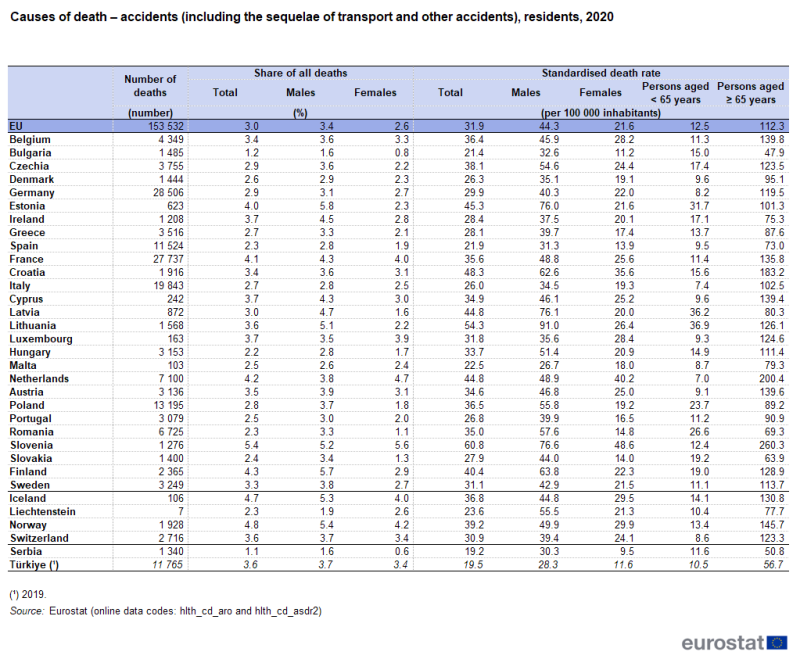
In 2020, there were 153 500 deaths in the EU resulting from accidents, equivalent to 3.0 % of all deaths among residents. In Slovenia, Finland, the Netherlands, France and Estonia (among the EU Member States), as well as in Norway and Iceland (among the EFTA countries), the proportion of deaths from accidents in 2020 was at least 4.0 %. The highest share among the EU Member States was recorded in Slovenia (5.4 %), which was 1.1 percentage points higher than in Finland (which recorded the second highest share; 4.3 %). Accidents accounted for less than 2.0 % of all deaths in Bulgaria (1.2 %); this was also the case in Serbia (among the candidate countries; 1.1 %).
Source: Eurostat (hlth_cd_aro) and (hlth_cd_asdr2)
In 2020, a higher share of deaths among men (than among women) in the EU were from accidents (3.4 % compared with 2.6 %). This pattern was repeated across all of the EU Member States except for Luxembourg, Slovenia and the Netherlands, where the share among women was higher than that among men; this was also the case in Liechtenstein. The most pronounced gender differences were in the Baltic Member States where the differences between the sexes – with higher shares among men – were at least 2.9 percentage points.
Men more likely than women to die from all types of accidents
The EU’s standardised death rate for accidents was 31.9 deaths per 100 000 inhabitants in 2020. The death rate for men (44.3 per 100 000 male inhabitants) was just over double that for women (21.6 per 100 000 female inhabitants) – see Table 1. In all EU Member States, the standardised death rate for men in 2020 was higher than that for women, most notably in the Baltic Member States, Romania and Finland where the difference was more than 40 deaths per 100 000 inhabitants.
While accidents were a more common cause of death at advanced ages, the difference between standardised death rates for people aged less than 65 years and those aged 65 years and over was relatively narrow compared with other causes of death. The EU’s standardised death rate from accidents for those aged 65 years and over was nine times as high as the rate for persons aged less than 65 years; for all causes of death the standardised death rate for those aged 65 years and over was 22 times as high as for the younger age group.
A more detailed analysis of causes of death is presented in Table 2 for a selection of accidents, as well as assault. Among men and women, the three leading causes of death from accidents were falls, the miscellaneous category of other accidents (including, for example, burns, electrocution, crushing and overexertion) and transport accidents. For the causes of death shown in this table, standardised death rates in 2020 for women were rarely higher than those for men. The only exceptions among the EU Member States were assault in Slovenia and Austria, and other accidents in Malta.
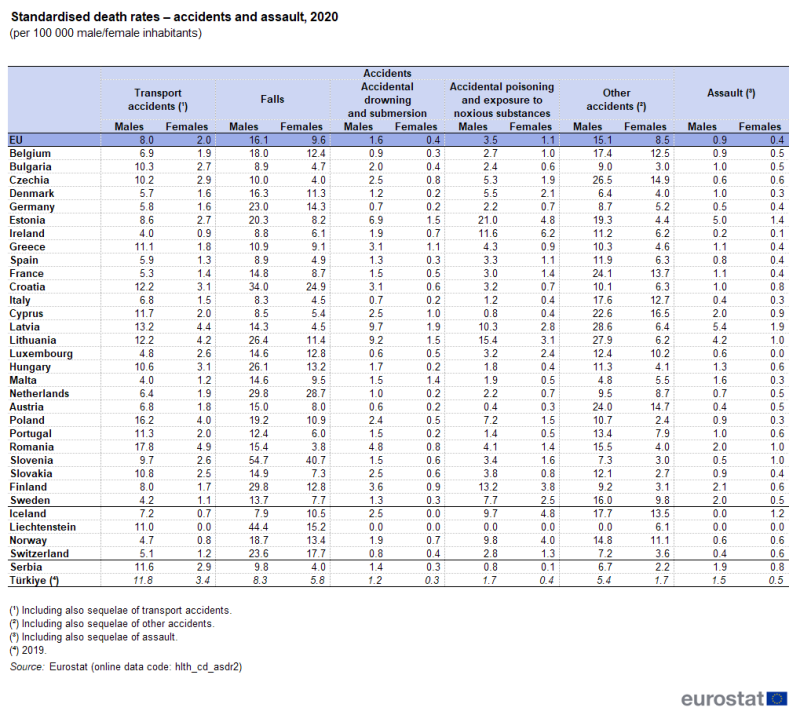
(per 100 000 male/female inhabitants)
Source: Eurostat (hlth_cd_asdr2)
In 2020, there were particularly high standardised death rates for some of these types of accidents in several individual EU Member States.
- For transport accidents, standardised death rates for men and for women were more than twice as high as the EU average in Romania; this was also the case for men in Poland and for women in Latvia and Lithuania.
- For falls, standardised death rates among women were more than four times as high as the EU average in Slovenia, and more than twice as high in the Netherlands and Croatia. Among men, the highest death rates were recorded in the same three EU Member States, peaking at more than three times as high as the EU average in Slovenia.
- For accidental drowning and submersion, standardised death rates for men and for women in the Baltic Member States were more than three times as high as the EU average, peaking in Latvia. This rate was also more than three times as high as the EU average for women in Malta.
- For accidental poisoning and exposure to noxious substances, standardised death rates for men were more than four times as high as the EU average in Lithuania and were six times as high in Estonia; among women, standardised death rates were more than four times as high as the EU average in Estonia and were 5.5 times as high in Ireland.
The highest standardised death rates for assault among males were in the Baltic Member States
In 2020, 2 977 people died from assaults in the EU, equivalent to 0.06 % of the total number of deaths. The standardised death rate for assault was 0.7 per 100 000 inhabitants across the EU, with the rate for males approximately twice as high as for females (0.9 deaths per 100 000 male inhabitants compared with 0.4 deaths per 100 000 female inhabitants). Among males, the highest standardised death rates for assaults in the EU Member States were recorded for the Baltic Member States, each recording rates that were at least 4.7 times as high as the EU average. Among females, rates that were at least twice as high as the EU average were observed in the Baltic Member States, as well as Slovenia and Romania.
Standardised death rates for assault in 2020 were generally higher among males than females, although the rate for females was slightly higher than that for males in Slovenia and Austria. The most pronounced gender differences were observed in the Baltic Member States, where the difference between the sexes – higher rates for men – was more than 3.0 deaths per 100 000 inhabitants.
Analysis by age for deaths from accidents
On the one hand, accidents may trigger a fatal deterioration in the health of older people: more than two thirds (70.5 %) of all deaths from accidents in the EU in 2020 were among people aged 65 years and over. On the other hand, a relatively high proportion of people under the age of 65 years die from accidents: the share of deaths caused by accidents was more than twice as high for people aged less than 65 years (5.8 %) as it was for people aged 65 years and over (2.5 %).
For all five-year age groups between the ages of 15 and 34 years, accidents were the single most common cause of death in the EU (when comparing with the other major categories in the 10th revision of the international statistical classification of diseases and related health problems (ICD-10); this was also the case for young people aged between 1 and 4 years. In 2020, accidents accounted for more than one third (33.7 %) of all deaths in the EU among people aged 15–19 years (see Figure 1) and for between one quarter and one third of all deaths among people aged 20–24 years and 25–29 years.
Looking across the age groups from youngest to oldest, there was a large jump in the number (and also the share) of deaths from accidents when moving from the age group 10–14 years to the age group 15–19 years: there were 4.2 times as many deaths from accidents in the older of these two age groups than in the younger one. This large jump can, in part, be attributed to deaths from transport accidents, which alone accounted for more than one fifth (21.3 %) of all deaths among people aged 15–19 years.
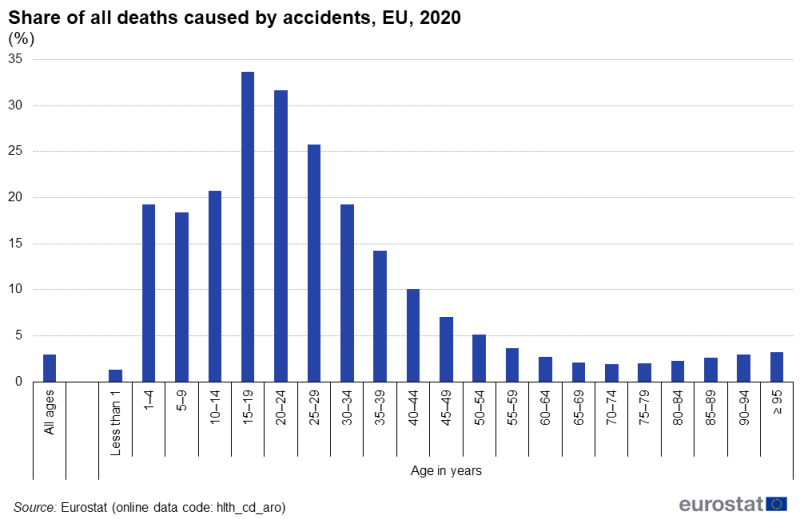
(%)
Source: Eurostat (hlth_cd_aro)
Analysis by age for deaths from assaults
Compared with accidents, the age profile of people in the EU dying from assaults was even more skewed away from older people: more than four fifths (82.0 %) of people killed by assaults in 2020 were aged less than 65 years. The five-year age range with the highest number of deaths from assaults was for people aged 40–44 years, some 273 deaths from assaults in 2020. Nevertheless, as a share of the total number of deaths within each age group, deaths from assaults were most common for the age group 20–24 years (2.2 % of all deaths for this age group).
The extent of accidents
Figures 2 and 3 present data for 2019. The information is derived from the third wave of the European health interview survey (EHIS) which covered persons aged 15 years and over. The survey included questions asking about injuries resulting from: i) transport accidents, ii) accidents at home, or iii) accidents while undertaking leisure activities, during the 12 months prior to the survey.
In 2019, some 7.1 % of the EU population (aged 15 years and over) reported that they had an accident (during the 12 months prior to the survey), at home or during a leisure pursuit, that resulted in an injury. At the lower end of the range, shares of less than 3.5 % were recorded in Poland and Romania, as well as Bulgaria (that had the lowest proportion among the EU Member States, at 2.3 %). By contrast, double-digit shares were observed in six Member States, with the highest shares in Finland (12.2 %), Czechia, Austria and Germany (all within the range of 11.8–11.9 %).
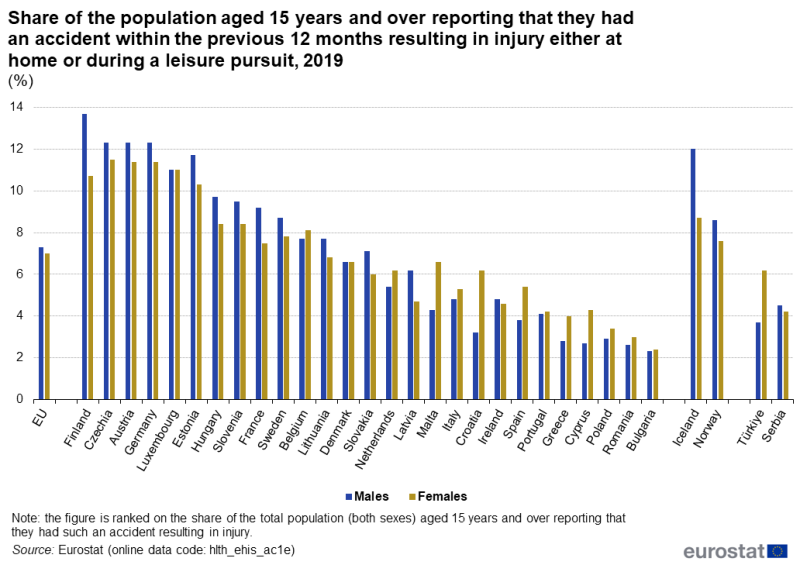
(%)
Source: Eurostat (hlth_ehis_ac1e)
In 2019, there were 13 out of 27 EU Member States where a higher proportion of males (than females) reported that they had an accident resulting in injury either at home or during a leisure pursuit; there was no difference between the sexes in Denmark and Luxembourg, while for the remaining 12 Member States a higher proportion of females reported injuries. The biggest gaps between the sexes were recorded in Finland and Croatia. In Finland, the share for males was 3.0 percentage points higher than for females, whereas the opposite was true in Croatia (as the share for females was 3.0 points higher than for males).
Accidents at home or during a leisure pursuit were more frequently reported by the youngest and oldest generations
An analysis by 10-year age ranges shows that the proportion of people in the EU who reported that they had been injured in an accident at home or during a leisure pursuit tended to be relatively high among youths (15–24 years), falling for people in middle age, before increasing again later in life.
- Among the EU Member States, the highest shares of people reporting an injury in 2019 were often youths; this was most notably the case in Germany (where 23.9 % of people aged 15–24 years had an accident at home or during a leisure pursuit that resulted in injury), Austria (19.6 %) and Luxembourg (18.0 %). For those Member States where this was not the case, it was common for people aged 75 years and over to record the highest share. There were only two exceptions, as the highest proportions of people reporting an injury in Finland and Lithuania were those aged 25–34 years.
- The lowest shares of people reporting an injury in 2019 were often recorded among people aged 55–64 years or 65–74 years. Bulgaria, Cyprus and Poland were notable exceptions, as their lowest shares were recorded for people aged 15–24 years.
Road traffic accidents most frequently reported by younger people
Across the EU Member States, the share of people (aged 15 years and over) reporting in 2019 that they had been injured in a road traffic accident (during the 12 months prior to the survey) was systematically lower than the share reporting they had been injured following an accident at home or during a leisure pursuit. The proportion of people injured in a road traffic accident ranged from lows of 0.2 % and 0.3 % in Romania and Bulgaria, respectively, up to highs of 2.2 % in Germany and 2.4 % in Belgium.
There was a fairly clear gender difference for road traffic accidents across the EU Member States, with males generally more likely than females to report that they had an injury from a road traffic accident in 2019. In Denmark, the proportions were the same for both sexes, whereas in Lithuania, Portugal, Finland, Latvia and Luxembourg the proportion was higher for females.

(%)
Source: Eurostat (hlth_ehis_ac1e)
An analysis by age for road traffic accidents shows a different pattern to that observed for accidents at home or during a leisure pursuit. For the EU, the highest share of people in 2019 reporting that they had been injured in a road traffic accident was 2.7 % among youths (aged 15–24 years). By contrast, the lowest shares were recorded among people aged 65–74 years and people aged 75 years or over (both 0.8 %).
For a small majority of EU Member States, the highest share of people reporting that they had been injured in a road traffic accident was recorded among youths. By contrast, in Bulgaria the joint highest proportions were registered in the three 10-year age groups from 35–44 years to 55–64 years, while in Czechia the highest proportion was among those aged 45–54 years. The lowest shares tended to be reported for older people (those aged 65–74 years or those people aged 75 years or over).
Healthcare for injuries, poisoning and other consequences of external causes
Austria, Germany and Bulgaria had the highest number of in-patient discharges for patients treated for accidents and injuries (relative to population size)
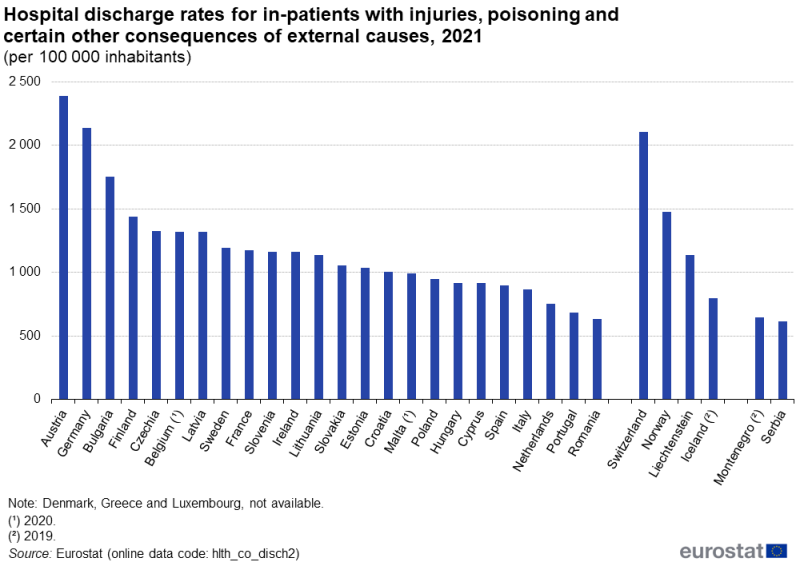
There were around 5.4 million in-patients with injuries, poisoning and certain other consequences of external causes (ICD codes S00–T98; hereafter referred to as accidents and injuries) discharged from hospitals in the EU in 2021 (2020 data for Belgium and Malta; no recent data for Denmark, Greece and Luxembourg). In-patient discharges of those treated for accidents and injuries accounted for at least 10.0 % of the total number of in-patient discharges in Austria and Finland, while they accounted for just 6.0 % in Bulgaria and 4.8 % in Romania.
Relative to population size, Austria, Germany and Bulgaria recorded the highest number of in-patient discharges for those treated for accidents and injuries (see Figure 4 for data availability), with 2 389, 2 140 and 1 752 per 100 000 inhabitants, respectively. The lowest ratios, among the EU Member States, were recorded in Portugal and Romania (683 and 634 per 100 000 inhabitants, respectively).
(per 100 000 inhabitants)
Source: Eurostat (hlth_co_disch2)
Particularly long average length of stay for in-patients with a fracture of the femur
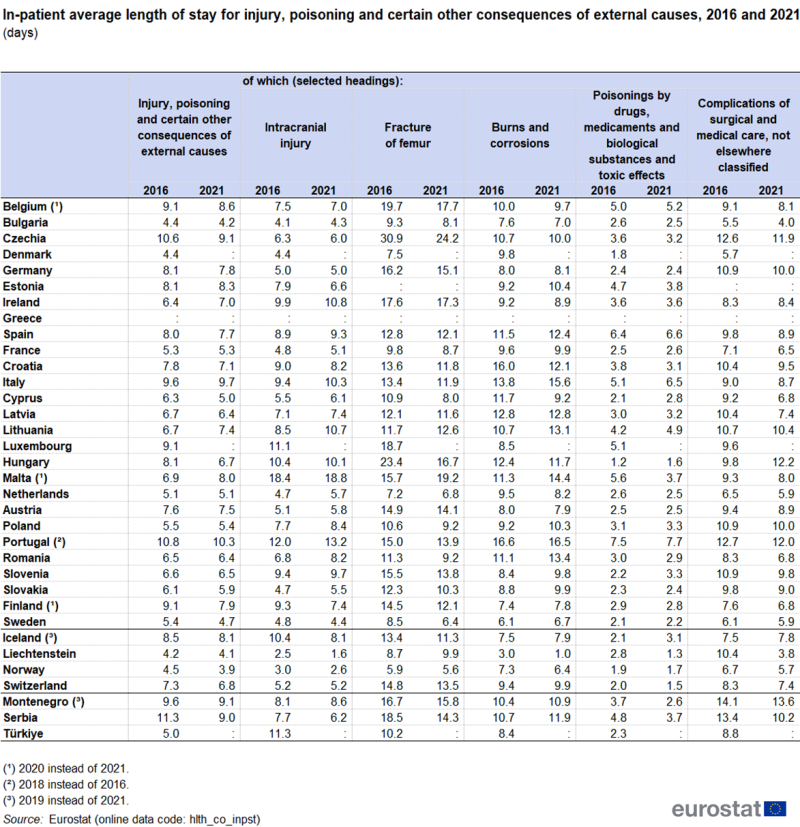
Across the EU, in-patients with accidents and injuries spent a total of 38.8 million days in hospital in 2021 (2020 data for Belgium and Malta; no recent data for Denmark, Greece and Luxembourg). An analysis of the average length of hospital stays for in-patients treated for injuries, poisonings and certain other consequences of external causes shows that, in 2021, this figure generally ranged from 4.2 days in Bulgaria up to 8.3 days in Estonia: above this range, averaging 8.6, 9.1, 9.7 and 10.3 days, respectively, were Belgium (2020 data), Czechia, Italy and Portugal. Comparing the average length of stay in 2016 with that in 2021 (see Table 3 for data availability), most EU Member States reported increases or decreases of less than 1.0 days. Czechia, Hungary, Cyprus and Finland (2016–2020) recorded larger decreases, while Malta (2016–2020) recorded a larger increase.
(days)
Source: Eurostat (hlth_co_inpst)
Table 3 also provides a more detailed analysis of the average length of hospital stays for in-patients diagnosed with five different types of accidents and injuries. In-patients with a fracture of the femur (code S72) tended to spend the highest average number of days in hospital, whereas those poisoned by drugs, medicaments and biological substances or treated for toxic effects (codes T36–T65) generally spent the lowest average number of days in hospital.
Source data for tables and graphs
Data sources
Key concepts
An in-patient is a patient who is formally admitted (or ‘hospitalised’) to an institution for treatment and/or care and stays for a minimum of one night or more than 24 hours in the hospital or other institution providing in-patient care. An in-patient or day care patient is discharged from hospital when formally released after a procedure or course of treatment (episode of care). A discharge may occur because of the finalisation of treatment, signing out against medical advice, transfer to another healthcare institution, or because of death.
The number of deaths from a particular cause of death can be expressed relative to the size of the population. A standardised (rather than crude) death rate can be compiled which is independent of the age and sex structure of a population: this is done as most causes of death vary significantly by age and according to sex and the standardisation facilitates comparisons of rates over time and between countries.
Healthcare resources and activities
Statistics on healthcare activities (such as information on hospital discharges) are documented in this background article which provides information on the scope of the data, its legal basis, the methodology employed, as well as related concepts and definitions.
For hospital discharges and the length of stay in hospitals, the international shortlist for hospital morbidity tabulation (ISHMT) is used to classify data from 2000 onwards; Chapter XIX covers injury, poisoning and certain other consequences of external causes.
- Intracranial injury (1901)
- Other injuries to the head (1902)
- Fracture of forearm (1903)
- Fracture of femur (1904)
- Fracture of lower leg, including ankle (1905)
- Other injuries (1906)
- Burns and corrosions (1907)
- Poisonings by drugs, medicaments and biological substances and toxic effects of substances chiefly nonmedicinal as to source (1908)
- Complications of surgical and medical care, not elsewhere classified (1909)
- Sequelae of injuries, of poisoning and of other consequences of external causes (1910)
- Other and unspecified effects of external causes (1911)
For country specific notes on these data collections, please refer to the annexes at the end of the national metadata reports accessible from links at the beginning of the European metadata report.
The Healthcare non-expenditure statistics manual provides an overview of the classifications, both for mandatory variables and variables provided on voluntary basis.
Health status (extent of injuries)
Self-reported statistics covering the health status of the population for a range of chronic diseases are provided by the European health interview survey (EHIS). This source is documented in more detail in the background article European health interview survey – methodology which provides information on the scope of the data, its legal basis, the methodology employed, as well as related concepts and definitions. The data presented in this article refer to the share of the population aged 15 years and over reporting that they had been injured through transport accidents, accidents at home, or while undertaking leisure activities during the 12 months prior to the survey.
Causes of death
Statistics on causes of death provide information on mortality patterns, supplying information on developments over time in the underlying causes of death. This source is documented in more detail in this background article which provides information on the scope of the data, its legal basis, the methodology employed, as well as related concepts and definitions.
Causes of death are classified according to the European shortlist (86 causes), which is based on the International Statistical Classification of Diseases and Related Health Problems (ICD). Chapter XX of the ICD covers external causes of morbidity and mortality.
- V01–X59 Accidents
- V01–V99 Transport accidents
- W00–X59 Other external causes of accidental injury
- W00–W19 Falls
- W65–W74 Accidental drowning and submersion
- X40–X49 Accidental poisoning by and exposure to noxious substances
- Other accidents
- W20–W49 Exposure to inanimate mechanical forces
- W50–W64 Exposure to animate mechanical forces
- W75–W84 Other accidental threats to breathing
- W85–W99 Exposure to electric current, radiation and extreme ambient air temperature and pressure
- X00–X09 Exposure to smoke, fire and flames
- X10–X19 Contact with heat and hot substances
- X20–X29 Contact with venomous animals and plants
- X30–X39 Exposure to forces of nature
- X50–X57 Overexertion, travel and privation
- X58–X59 Accidental exposure to other and unspecified factors
- X85–Y09 Assault
- Y85–Y89 Sequelae of external causes of morbidity and mortality
- Y85 Sequelae of transport accidents
- Y86 Sequelae of other accidents
- Y87 Sequelae of intentional self-harm, assault and events of undetermined intent
- Y87.1 Sequelae of assault
Important note: for the statistics presented in this article, deaths from the sequelae of transport accidents are included under transport accidents, deaths from the sequelae of other accidents are included under other accidents. Equally, deaths from the sequelae of assault are included under assault. Sequelae denotes a chronic condition resulting from a certain disease or injury.
Symbols
Tables in this article use the following notation:
| Value in italics | estimate or provisional data; |
| Value is : | not available. |
Context
With 153 500 deaths in 2020 (3.0 % of all deaths), accidents were the one of the most common causes of death in the EU, underlining the importance of policy actions that are designed to prevent accidents/injuries.
Research evidence suggests many accidents are preventable. In June 2006, the European Commission adopted a Communication on Actions for a safer Europe (COM(2006) 0328 final) emphasising prevention measures. In May 2007, a Council Recommendation on the prevention of injury and the promotion of safety was adopted, targeting seven key priority areas, namely: the safety of children and adolescents; elderly citizens; vulnerable road users; the prevention of sports injuries; injuries caused by products and services; self-harm; and interpersonal violence.
One of the actions conducted as part of the EU’s health programme for 2008–2013 was a joint action on monitoring injuries in Europe (JAMIE). The overall objective of JAMIE was, by the end of 2013, to have a common hospital-based injury surveillance system in operation in the majority of EU Member States. JAMIE aimed to refine the methodology for collecting hospital-based injury data with a view to facilitate data collection and incorporate countries into the European injury database (IDB) monitoring system and exchange mechanism. The joint action offered assistance such as standardised training for national data administrators, twinning programmes, on-site consultations and country specific coaching for EU Member States which needed to start or restart a system, as well as continuous supervision and joint monitoring actions concerning the level of implementation in each Member State.
link







